 Skip to content
Skip to content
Total hip replacement (THA) is one of the most successful surgeries. Both modern cemented and uncemented femoral components have shown excellent efficacy in the practice. The Charnley Cemented Low Friction Arthroplasty was the first implant to have a high survival rate. However, in the early stages of their development, cemented prostheses had poor survival rates due to poor implant design and bonding techniques. This led to the development of cementless prostheses.
Basic Science of Cementless Fixation
Osseointegration is the direct connection of bone to the surface of an artificial implant. Although osseointegration has been described as involving different metals, it is commonly used to describe the fusion of bone with titanium.
In 1940, scientists first described the phenomenon, and in 1952, they accidentally discovered that a titanium implant placed in a rabbit’s leg fused to the bone, coining the term “osseointegration.” Titanium implants are mechanically stabilized and chemically retained in the bone through direct contact of calcium atoms with the titanium oxide surface, creating a purely inorganic interface, resulting in pure osseointegration. Cobalt-chromium alloys are also commonly used, however, titanium is more biocompatible and its elasticity is closer to that of bone, resulting in less thigh pain and stress shielding.
Proper bone contact and fixation minimize micromotion and prevent fibrous ingrowth. Micromovements >150mm will lead to the formation of fibrous tissue, micromovements of 30~150mm will lead to the formation of bone and fibrous tissue, and micromovements <28mm will lead to major bone formation. The porous implant structure allows extensive bone infiltration with vascularization and osteoblastic activity within the implant. Osseointegration can occur through bone ingrowth or growth, depending on the surface characteristics of the implant.
Ingrowth refers to the growth of bone into the porous surface of the implant; ingrowth occurs when bone grows over the rough surface of the implant. Growth requires implant pore diameter between 50-400mm and porosity 40% – 50%. Ingrown surfaces include sintered beads, fiber mesh, and porous metals. The growth surface is formed by sandblasting or plasma spraying. Hydroxyapatite (HA) is an osteoconductive agent used as an auxiliary in porous coatings and sandblasted surfaces. Regardless of the fixation surface, it should be circumferentially continuous to enhance osseointegration, reduce failure rates, and prevent wear particle migration.
Common types of biological femoral stems
The design of the cementless stem determines the contact point between the implant and cortical bone, resulting in differences in biomechanics and fixation between implants. The aim is to achieve initial stability through maximal primary fixation and adequate bony contact, followed by secondary biologic fixation.
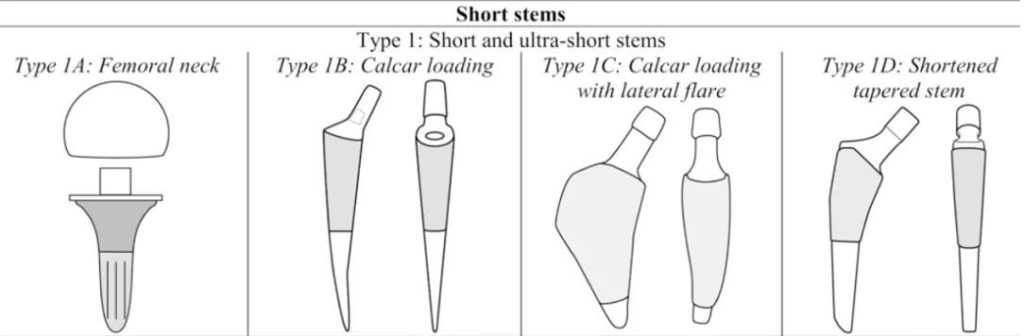
Type 1A: Femoral Neck: Type 1A femoral stem is only used for femoral neck fixation. Primary stability is achieved through cancellous bone compression.
Type 1B: Calcar-Loading Stem. These are cervical-sparing stalks that extend into the metaphysis. They achieve fixation at the femoral calcar and proximal femoral cortex
Type 1C: Calcar-Loading Stem with Lateral Flare, these stems have a lateral flare that provides fixation to the lateral cortex and calcar and allows for load distribution of the proximal femur
Type 1D: Shortened Tapered Stem. These stems are similar to traditional proximally coated tapered stems, but have a shorter distal taper to avoid stress shielding and typically extend only to the proximal end of the diaphysis, designed for proximal stress transfer.
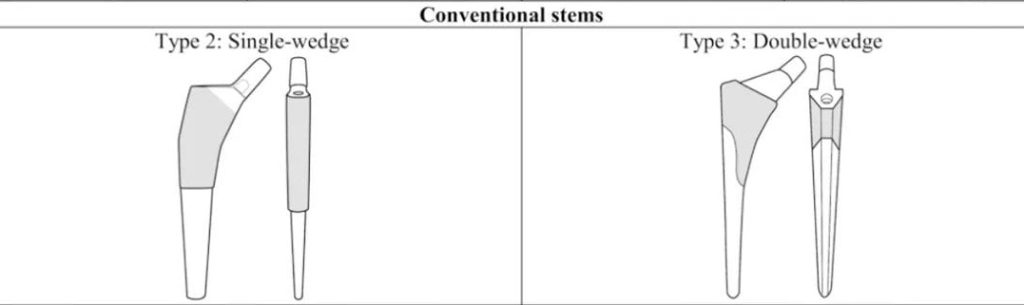
Type 2: Single-Wedge (Single Taper) Stem:
The type 2 stem joins the metaphysis only on the medial plane and is flat and elongated on the anterior and posterior planes. It is thin anteriorly and posteriorly, and narrows internally and externally, with proximal coating and metaphyseal fixation. It is suitable for the medullary cavity shape of the Dorr-B type femur. It should be used with caution for Dorr-A type femur and Dorr-C type femur in elderly patients.
Type 3: Double-Wedge (Dual Taper), Metaphyseal-Filling Stem: Type 3 stems involve the proximal femur in both the medial and lateral femoral and anteroposterior planes. The proximal end is wider and thicker than the single wedge handle front and rear, and the distal end is narrowed both inner and outer as well as front and rear. The proximal end is filled and fixed, and the filling of the backbone is helpful in enhancing rotational stability
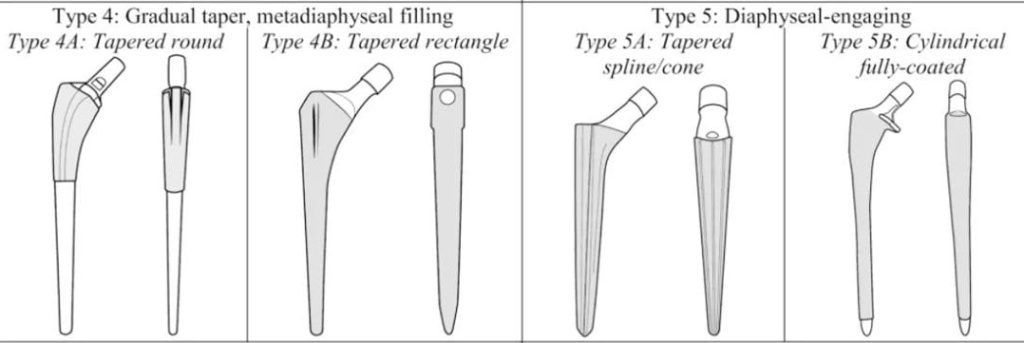
Type 4: Gradual Taper, Metadiaphyseal-Filling Stem:
The Type 4 stem has a smooth and gradual taper in the anteroposterior and medial-lateral planes, rather than a steep taper, and is anchored to the metaphysis. Two subtypes are described: tapered round stem (type 4A), porous coating on the proximal 2/3, tapered, oval, metaphyseal-diaphyseal junction fixation. Tapered rectangular handle (Type 4B), rectangular cross-section, 4-point rotational support in the metaphyseal and diaphyseal areas, and fixation at the junction of the metaphyseal end and diaphysis and the proximal diaphysis.
Type 5: Diaphyseal-Engaging Stem:
These prostheses are suitable for proximal hip joints that are difficult to fix and are usually suitable for hip revision or primary total hip replacement with proximal bone loss. There are two types of backbone-engaging stems, Type 5A stems, and tapered grooved stems. Conical shape, with longitudinal ridges, fixation at the junction of metaphysis and diaphysis and proximal diaphysis, emphasizing the importance of trial molding and medullary cavity preparation, with a rough surface, and the stem is designed to wedge into the femoral medullary canal to provide axial direction and flexural stability, the rough surface allows bone growth. Type 5B stem, cylindrical stem, extensively coated, the proximal collar can improve proximal bone load and axial stability, distal fixation, mainly relies on “rubbing” fixation of the femoral shaft, and the prosthesis relies on the initial fixation of the entire prosthesis, in patients with missing proximal femurs, diaphyseal moderation, and filling are critical to initial stability.
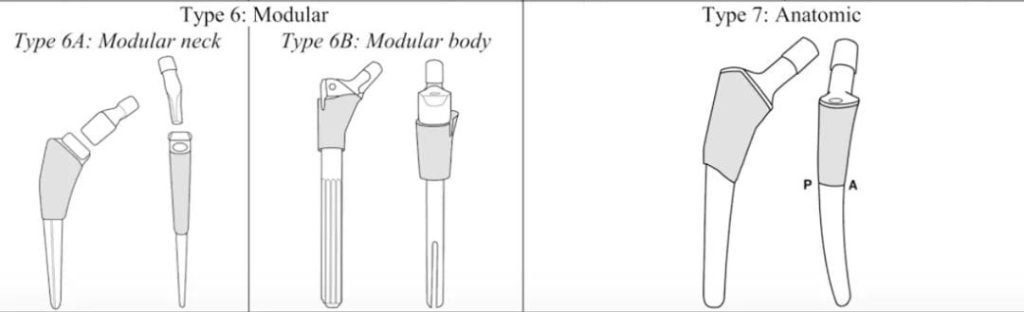
Type 6: Modular Stem:
The combined use of the femoral neck and femoral shaft allows the limb length, neck shaft angle and anteversion angle to be freely adjusted, which is beneficial to the biomechanical reconstruction of the hip joint and is suitable for some complex hip replacement types. There are several theoretical advantages, including the ability to fine-tune anteversion, length, and offset, but disadvantages include corrosion at the assembly interface when micromotion occurs, which can lead to adverse local tissue reactions and higher costs.
Type 7: Anatomic Stem:
With a broad posterolateral aspect of the proximal portion, a posterior arch at the metaphysis and an anterior arch at the diaphysis, these stems are bent posteriorly at the metaphysis so that they are parallel to the endosteal geometry of the proximal femur and achieve maximum contact, while at the diaphysis they bend forward.
Conclusion:
Cementless systems are generally very successful regardless of their design. However, while short stems are increasingly popular, long-term results remain unknown. Additionally, modular implants carry the risk of corrosion and fatigue failure. Finally, uncemented fixation carries a higher risk of periprosthetic fractures, especially in older female patients. Therefore, the use of cemented or cementless stems should be individualized based on available evidence.