 Skip to content
Skip to content
Volar locking compression plate (LCP) internal fixation is the golden standard for the treatment of distal radius fractures, but LCP is not practical for all distal radius fractures, such as extreme distal radius fractures and dorsal edge fractures. Volar side die-punch fractures, etc. At the same time, LCP plates also have many complications, including pronator muscle injury, fracture blood supply disruption, volar soft tissue irritation, dorsal tendon wear, etc., And are also suitable for severe osteoporosis. Patients are at higher risk of internal fixation failure.
The need to reduce postoperative complications and reduce iatrogenic injuries has led to the development of various new internal fixation methods. This article briefly introduces 4 new internal fixation methods for the reference of clinicians.
| Type | Indications | Advantages | Disadvantages |
| Intramedullary nail | Extra-articular and simple intra-articular fractures | 1. Smaller incisions 2. Reduces risk of tendon injury and screw penetration into the joint 3. Minimizes soft tissue stripping while permitting early motion | Less distal fixation Increased risk for loss of reduction |
| Intramedullary cage | Extra-articular and simple intra-articular fractures | 1. Smaller incisions 2. Fixed angle fixation with subchondral 3. Support and load sharing Intramedullary placement of fixation construct 4. Minimizes soft tissue stripping | 1. Soft tissue irritation from prominent screws 2. Concerns related to bone loss during hardware removal in the setting of bone on growth |
| Radiolucent PEEK volar locking plate | Early motion and weight-bearing | 1. Modulus of elasticity similar to bone 2. Improved visualization of fracture reduction and bone healing 3. No risk of cold weld-ing between screws and plate 4. Low artifact interference with MRI and CT imaging | 1. Cannot be contoured locking screws create threads in the plate. 2. limiting the number of attempts at redirecting the screw 3. Concerns about excessive plate flexibility and plastic wear from screws Similar soft tissue and fixation-related problems to metallic volar locking plates |
| Distal radius hemiarthroplasty | Comminuted intra-articular fractures in elderly patients with osteoporotic bone, possible distal ulna fractures | 1. Cannot be contoured locking screws create threads in the plate. 2. limiting the number of attempts at redirecting the screw 3. Concerns about excessive plate flexibility and plastic wear from screws 4. Similar soft tissue and fixation-related problems to metallic volar locking plates | 1. Articular wear of the proximal carpal row 2. Carpal instability 3. Implant loosening 4. Increased bone loss lf foot salvage is required |
1. Distal radius intramedullary nail
Intramedullary nailing of the distal radius appeared relatively late. The intramedullary nail technology is widely used in long-bone diaphyseal fractures. Closed or limited open reduction can effectively reduce the damage to blood supply caused by iatrogenic factors and has good biological advantages of axial fixation. This technology is suitable for complete extra-articular fractures and simple intra-articular fractures but is not suitable for comminuted intra-articular fractures.

The prerequisite for intramedullary nail fixation of distal radius fractures is that the closed reduction effect is satisfactory. After temporary fixation, the Kirschner wire is inserted through the opening of the radial styloid process and into the first/second compartment space on the dorsal side of the wrist. Potential injuries associated with this technique include damage to the radial nerve branches, screw penetration into the distal radioulnar joint or radiocarpal joint.
2. Cage support technology
Cage support technology is widely used in the reduction and fixation of osteoporotic fractures, such as proximal humerus fractures. In the same way, this technology can also be applied to osteoporotic distal radius fractures. Theoretically, with minimal soft tissue dissection, Cage support can be inserted through a limited incision after reduction to achieve intramedullary support and effective subchondral support, and assist in screw fixation. However, this technique may not be suitable for patients with good bone mass, and implant removal is also difficult.


3. PEEK volar locking plates
PEEK volar locking plates have the following characteristics:
① No visualization under fluoroscopy, which is convenient for observing fracture reduction and evaluating fracture healing during surgery;
② Similar to the elastic modulus of bone cortex, avoiding stress shielding effect;
③ PEEK material and metal screws, avoid cold welding.
But at the same time, the PEEK steel plate non-development technology is not conducive to evaluating whether the internal fixation has failed, and the PEEK steel plate cannot cope with shaping, and the internal fixation strength is weakened after changing the screw direction.
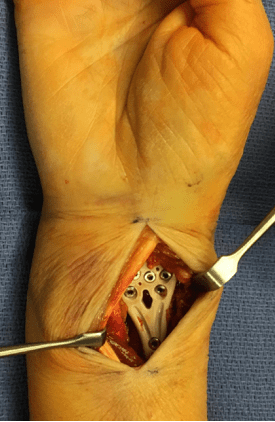

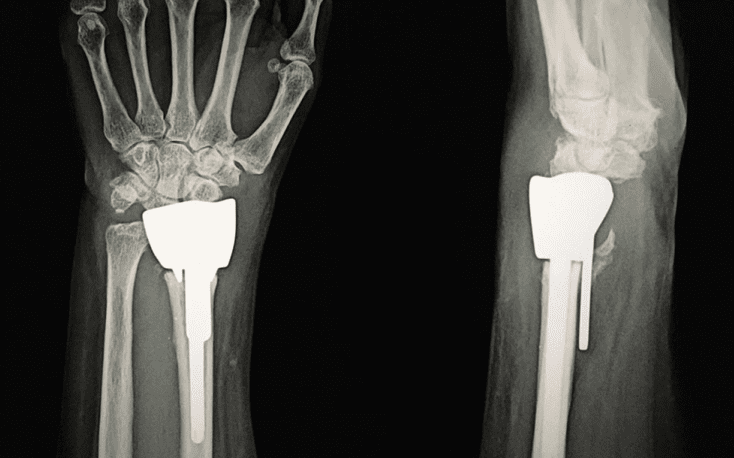
4. Distal radius joint replacement
Joint replacement for the treatment of severe intra-articular comminuted fractures has been applied to proximal humerus fractures, distal humerus fractures, tibial plateau fractures, etc. In the same way, joint replacement can also be used for distal radius fractures. It is suitable for the first-stage treatment of severe comminuted, intra-articular, and osteoporotic fractures, or the second-stage revision of internal fixation failure. Usually, a dorsal radial incision is used, entering from the 3rd/4th intercompartment.
In conclusion, the evolving landscape of internal fixation methods for distal radius fractures offers clinicians a broader spectrum of options tailored to specific patient needs. While the traditional Volar locking compression plate remains the gold standard for many cases, these innovative techniques provide valuable alternatives, especially for complex or osteoporotic fractures. Ultimately, the pursuit of improved outcomes and reduced iatrogenic injuries continues to drive progress in the field, benefiting both patients and practitioners alike.