 Skip to content
Skip to content
Intramedullary nailing is the most common treatment for femoral diaphysis fractures in adults. Proper preoperative assessment of fracture type, comminution, fracture extension, femoral length, and morphology is essential.
Several methods of direct and indirect estimation of femoral nail length have been described. Direct measurement of the contralateral intact femur (from the tip of the greater trochanter to the proximal patella) can serve as a rough guide but may be inaccurate in obese patients. Using X-rays can address this, but involves radiation exposure, and radiological magnification can lead to inaccuracies. Other methods include the use of intramedullary nail templates, fluoroscopy rulers, or Kuntscher bone measuring instruments. All of these approaches require an intact contralateral femur. For bilateral comminuted fractures, measurements are taken on the less comminuted side.
The intramedullary nail length can be measured as shown in the figure below during the operation:
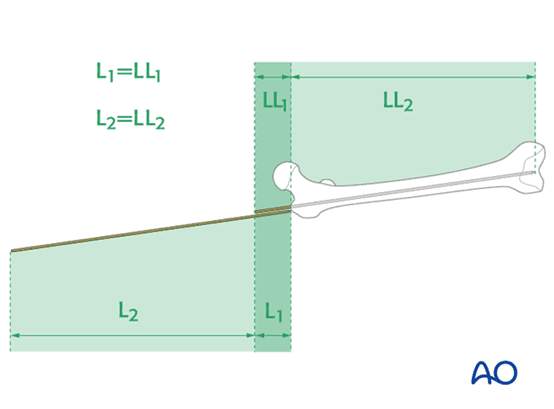
The correct length of the staple is determined intra-operatively by comparing the second guide wire with the already inserted guide wire. The correct position of the guide wire in the distal spinal canal should be assessed by fluoroscopy. Additionally, the second wire must be in contact with the greater trochanter. This has to be verified through perspective.
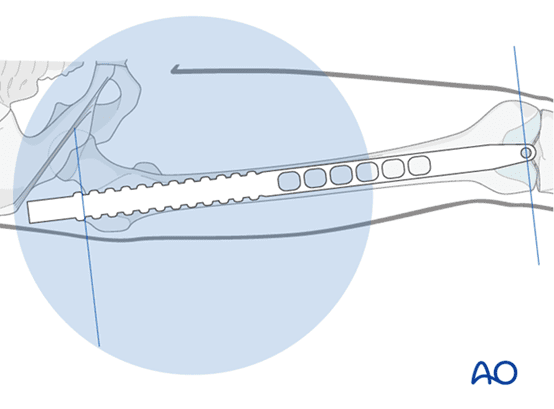
You can also use a perspective ruler. The tip of the ruler should be centered on the distal femur. The length of the intramedullary nail is determined by the position of the piriformis fossa, not by the tip of the greater trochanter.
Method 1: Length from the tip of the elbow to the little finger
Measuring the length of the forearm plus the little finger (from the tip of the olecranon to the tip of the little finger) is another way to determine the length of the femur. This study evaluated the correlation between forearm plus little finger length and femur length in 100 volunteers.
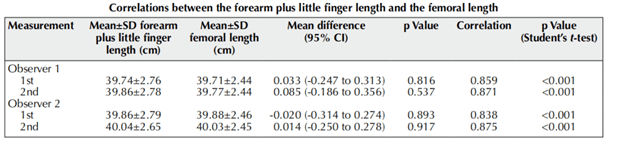
In this study, the correlation between the two measures was 0.86 (p<0.001), and it was not affected by age, sex, and BMI. The length of the forearm plus the little finger represents the maximum length of the femoral intramedullary nail. The method is simple, radiation-free, and can be applied in daily work.
Method 2: Length from the tip of the elbow to the thumb
We recruited 70 patients who underwent long radiographs of the lower extremities for other reasons and measured their forearms. We used a single dedicated measuring device for all patients consisting of a plastic plate with cm and mm increments clearly displayed. Measurements were taken from the tip of the olecranon to the tip of each finger with fingers adducted, forearm pronated, and elbow flexed to 90°.
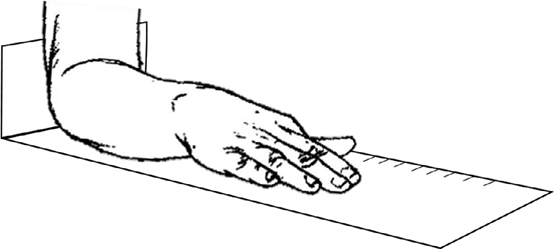
This is the instrument used to measure the olecranon to the fingertip. The forearm is pronated on the machine and the elbow is placed on the angle formed by the vertical and horizontal plates. Fingers are in the retracted position. Use the centimeter and millimeter markings on the level plate to measure.
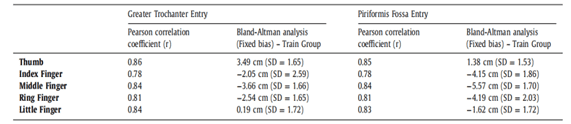
Data summary showing the Pearson correlation coefficients for all participants and the results of the Bland-Altman analysis for the thumb, index, middle, ring, and little fingers in the Train group only when compared with the maximum length of femoral nails at the greater trochanter and piriformis Fossa entrance.
The fixation bias (mean difference between elbow and x-ray measurements representing the greater trochanter (GT) approach) was 3.49 cm. The fixed bias of the entrance to the piriformis fossa (PF) was 1.38 cm. The following formula can be obtained:
Femoral nail length (GT) ≈ length from olecranon to thumb tip + 3.5cm
Femoral nail length (PF) ≈ length from olecranon to thumb tip + 1.4cm
We have shown that the length from the elbow joint to the tips of all five fingers has a strong correlation with the appropriate length of the femoral intramedullary nail. However, our study showed that, of all fingers, proper femoral nail length was most strongly associated with the previously unstudied elbow-thumb distance.
By simply measuring the distance from the elbow joint to the tip of the thumb, adding 3.5 cm if using the greater trochanter approach, with an increase of 1.4 cm if the piriformis fossa approach is used, the surgeon can confidently estimate the length of the femoral intramedullary nail used in a case, making it available prior to induction of anesthesia.
Method 3: Accurately predict the length of the femoral intramedullary nail from the patient’s height
In this study, a new linear regression equation was used to analyze 567 cases of femoral fractures in the past. We determined the new projected nail length based on the formula for the “optimal” nail length determined by x-ray. The corrected accuracy of this equation in anterograde and retrograde nails was determined. In addition, the number of times the equation predicts too long and too short is recorded. Validate the linear regression equation.
The linear regression equation between the intramedullary nail and the patient’s height is:
Antegrade intramedullary nail length = 178 × (patient height) + 85
Retrograde intramedullary nail length = 196 × (patient height) + 27
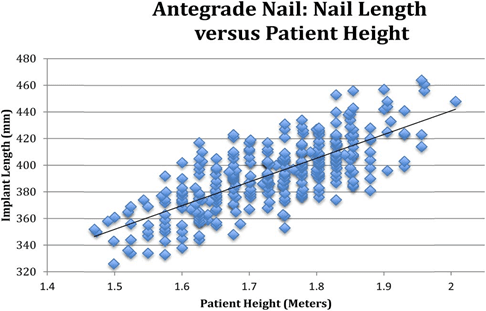
Data points for all anterograde spikes. Plot the patient’s intramedullary nail length versus the patient’s height. R = 0.55 (p<0.01).
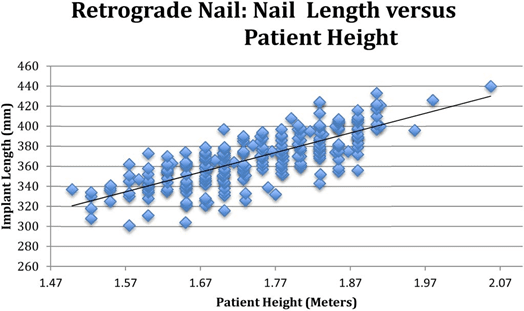
Data points for all retrograde spikes. Plot the patient’s nail length versus the patient’s height. R = 0.59 (p<0.01).
This measurement is always subject to a small amount of human error and may not reflect the absolute correct height of the patient. Considering most nails only add 20mm, this is an acceptable change. We propose 2 formulas to determine the exact length of the intramedullary nail according to the patient’s height. These equations should serve as valuable aids to improve the accuracy of choosing the correct intramedullary nail length.
Method 4: femoral intramedullary length = fibula length + femoral head diameter
The femoral length reference method includes the calculation of fibula length and femoral head diameter. The fibular length was defined as the distance between the proximal and distal ends of the bone. The femoral head diameter was defined as the longest distance between the medial inferior edge and the lateral superior edge of the femoral head. Femoral medulla length was defined as the vertical distance between the lateral fossa and the inter-condylar fossa.
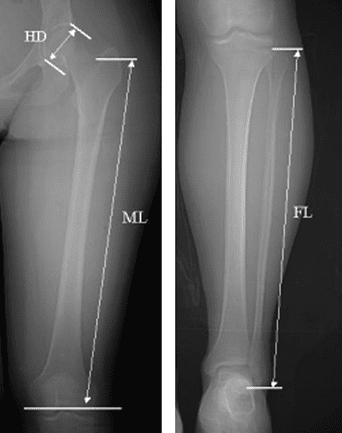
A representative digital x-ray view (CT map) of its measurements. Femoral head diameter (HD), femoral marrow length (ML), and fibula length (FL) were measured in the left lower extremity.
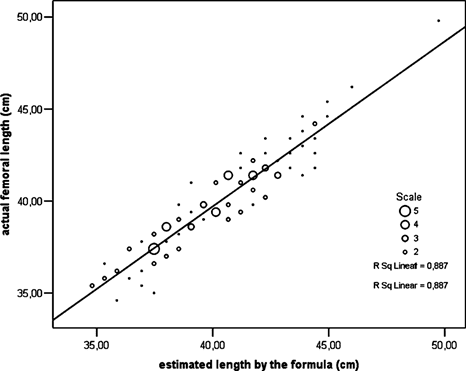
Scatterplot of actual femoral medulla length versus the sum of fibula length and femoral head diameter.
After estimating the medullary length, determine the length of the intramedullary nail. Ideally, the tip must be located some distance from the inter-condylar notch and away from the horizontal maxillary fracture. Subtract the distance from the inter-condylar notch to the distal end of the nail from the estimated medullary length. The result is the optimal length for anterograde nail fixation. A similar formula can also be used in retrograde nailing. The fibula length + femoral head diameter formula can be used as a simple and accurate estimation method of the actual femoral medulla length which cannot be measured in the contralateral femur. Therefore, it can be used for screw fixation, especially in the case of bilateral comminuted femoral fractures.
Conclusion
The above methods can roughly predict the length of the intramedullary nail before the operation. Some methods are simple and easy to implement. However, the actual selection of the length of the intramedullary nail depends on the actual situation of the operation during the operation. Selecting the appropriate length of the intramedullary nail is also a key step in the operation. Pre-estimating the length of the intramedullary nail also saves operation time, reduces the number of fluoroscopy times, and reduces surgical steps and other advantages, hoping to help clinicians make comprehensive preoperative planning.