 Skip to content
Skip to content
Is an acute ACL injury unsuitable for surgery? In addition to the reconstruction of the ACL repair method, what is the effect of ligament repair? Let me share with you about the past and present of ACL repair.
History of ACL repair
In 1900, two doctors quarreled over who was the first person in the world to undergo ACL repair surgery. The repair of the ACL was first known by William Battle in 1900 when he reported it in a journal. Sir Arthur Mayo-Robson claimed to have performed an ACL repair as early as 1895. The operation effect is surprisingly good. Mayo-Robson has followed up with the patients for 6 years, and his patients not only return to life but also return to sports.
After that, many doctors began to pursue this technology, such as Hubert Goetjes, who described 23 different types of ACL injuries and proposed corresponding surgical methods. Georg Perthes (discovered the Perthes disease, proposed the Perthes test to evaluate the ability of the deep femoral vein, and invented the cuff to drive blood before surgery) made some improvements to this technology, For example, copper and aluminum alloy wires are used to bind the ligament stump to the lateral femoral condyle, but it was eventually abandoned due to serious complications of joint stiffness.
As more and more people recognized ACL injuries and chronic cases gradually surfaced, repair techniques and reconstruction techniques began to flourish. Artificial ligaments were the first shots to be reconstructed: Dr. Fritz Lange reconstructed ligaments with fibers woven from silk in 1907, but unfortunately ended in failure. In 1917, Dr. Ernest William Hey Groves performed the first reconstruction of the ACL with the fascia lata. After that, various ligament reconstruction methods emerged in an endless stream, which can be called the golden age in the history of the ACL.
However, ligament repair technology has been under unprecedented siege. In 1976, Feagin et al. published a study on AJSM claiming that the 5-year failure rate was 50%. Since then, restoration technology has fallen into a downturn, while reconstruction technology has prevailed, beginning a 40-year dominance.
However, the repair technology did not die down and is still active in some areas. For example, in the case of an acute injury of the ACL with a patent epiphysis in adolescents, there is no shortage of repair techniques as a compromise solution. Moreover, the theory that the ACL has its own repair potential has been circulating in academic circles, and the voice of repair technology has never stopped.
In addition, doctors believe that the main reason for the poor long-term effect of repair technology is the wrong application of cases. For example, old ACL injuries, injuries near the middle or distal end of the ligament, and patients with too much activity, too young, and too fat should not use ligament repair in these cases. Van der List and DeFilice proposed a new classification based on the Sherman classification and believed that ligament avulsion near the femoral side and single-bundle ligament avulsion are better indications for ligament repair.
Ligament repair techniques
Ligament repair techniques have just caught up with technological advances. Spring-loaded, threaded anchors, cord reinforcement, and biological scaffolds have returned to people’s vision.
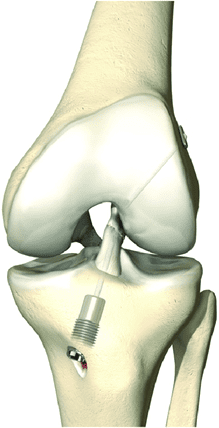
1. Spring Loaded Technology
Spring Loaded Technology appeared first. The results are as follows: the failure rate of single-cohort 1-year follow-up is 2.9%, the 2-year failure rate is 10%, the 5-year failure rate is 30%, and if you participate in strenuous exercise, the failure rate is 50%. Compared with ACL reconstruction, the 2-year failure rate is comparable. 60% of tibial implants need to be removed; this technique is currently only popular in some regions due to various registration restrictions
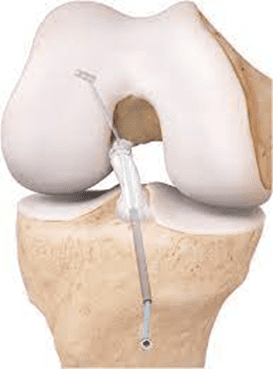
2. The threaded anchor technique
The threaded anchor technique can perfectly reproduce the double-bundle repair. It is not too difficult technically, and the record is also remarkable: Difelice et al. reported a cohort of 11 patients, and 2 patients failed after 3.5 years of follow-up; Achtnich adopted knot-free The method of anchor fixation combined with micro-fractures had a 1-year re-fracture rate of 15%; Overall, this technique has the advantages of low threshold, easy-to-use, no damage to the epiphysis, and less surgical trauma. However, there is insufficient contact surface between the ligament and the bone after the repair, the indications must be strictly grasped, and a longer period of recover after the operation.
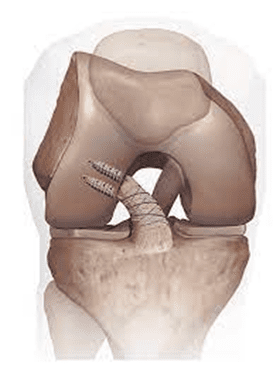
3. The cord reinforcement technology
The cord reinforcement technology can be said to be a cross-border player, like the artificial ligament version of the hamstring tendon, which provides high-strength support for its own ligament, and perfectly avoids the rough characteristics of the artificial ligament. The operator only needs to master the equidistant points of the ACL, basically, it is that simple. MacKay published a review of wire band technology, and the 2-year follow-up re-rupture rate in a 42-person cohort was 4.8%; Douoguih reported that in patients with an average age of 27.4 ± 8.6 years, the average follow-up time was 2-3.8 years, and the failure rate was 15%. %; if the patient’s age is increased, such as Schneider’s research found that when the patient’s age is between 30-56 years old, the failure rate of the follow-up time of 21 months is 3%; while the young and active population uses the wire-band technique to follow-up After 3 years, it was found that the cumulative re-fracture rate was 48.8%. So young and active is the nightmare of all repair techniques.
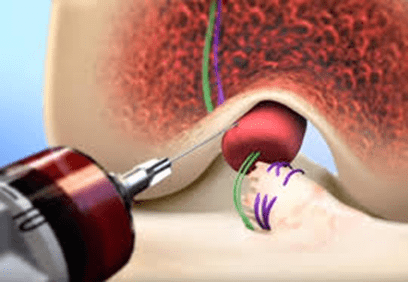
4. The biological scaffold
The biological scaffold is a high-end technology. First, bind the stump of the anterior cruciate ligament; second, stuff the femoral footprint into the bio-stent; third, extract your own blood and inject it into the bio-stent, and then tighten the ligament stump and let it grow when passing through the bio-stent.
In fact, in recent years, the treatment plan for ACL injury has been innovative. Sports rehabilitation is a new trend, it is pointed out that one-third of patients with ACL injuries can return to sports through rehabilitation training, some studies have also found that rehabilitation alone can restore the shape of the ligament in MRI. Even more surprisingly, there may be a high degree of overlap between patients who are eligible for rehabilitation and patients who are eligible for ACL repair.

The Canwell Cloud Endobuttons offer a comprehensive solution for acromioclavicular joint injuries. Featuring the innovative Xiangyun board with an adjustable fixed coil, these end buttons ensure precise and adaptable fixation. Their double titanium plate fixation conforms seamlessly to the anatomical and mechanical environment while providing elastic, non-rigid stabilization. The absence of a bone tunnel guarantees exceptional strength, and a specialized coracoid thread-passing device simplifies threading under the coracoid process. With a fusiform shape for easy insertion and a side opening hole for direct wire hanging, the low-incision design minimizes discomfort. Additionally, the horizontal 4-hole design accommodates preset adjustable or self-made adjustments, with suture knots securely fixed on the fibular side without tunneling. This elastic fixation aligns with anatomical mechanics, allowing weight-bearing without implant removal, thus avoiding further surgery. A specialized thread-passing tool simplifies wrapping the thread around the fibula, making the procedure simple and convenient.
Conclusion
All in all, the history of ACL repair and reconstruction techniques has been marked by continuous advancements and setbacks. Technological advances have brought back ligament repair methods. Although ACL repair technology is actively developing, it is important to continue to innovate considering the impact of the growing number of new technologies.