 Skip to content
Skip to content
With the extension of life span, the incidence of intertrochanteric fractures in the elderly continues to increase, and the goal of surgical treatment is to restore ambulation activities through early stable fixation. Currently, various fixation devices can be used to treat intertrochanteric fractures, among which PFNA is a commonly used fixation device. The PFNA-II has a helical blade with a locking mechanism, which is better at resisting rotation and providing stability compared to other instruments. Several authors reported excellent clinical results with PFNA-II, but the mismatched helical blade design raised concerns. This study aimed to review the clinical outcomes of proximal intramedullary nail herniation after the use of PFNA-II in patients with intertrochanteric fractures.
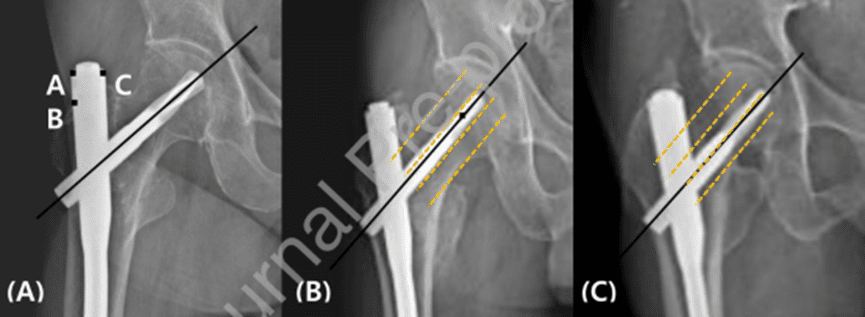
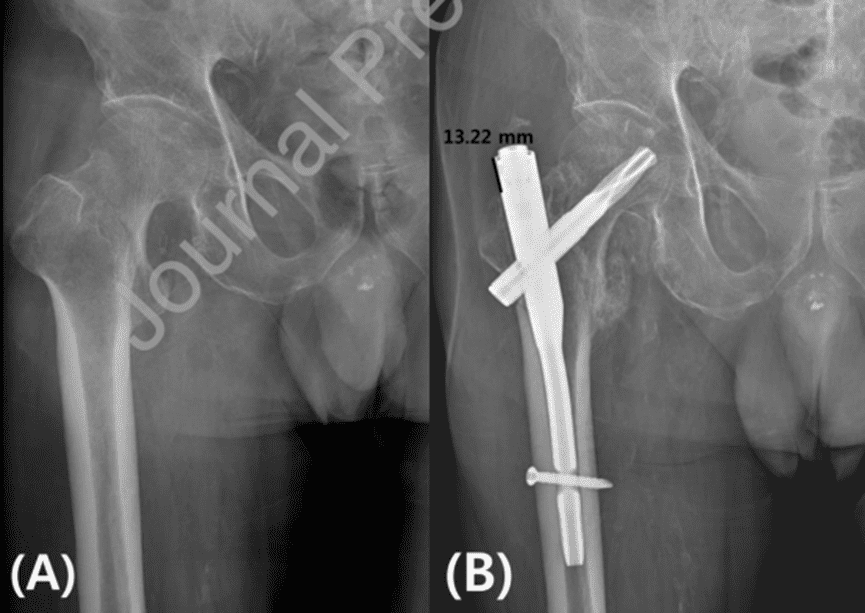
A retrospective analysis was conducted on 315 patients with intertrochanteric fractures who received PFNA-II treatment in our hospital from September 2010 to June 2018. All surgeries were performed by a single surgeon, and closed reduction was performed first after traction. When the C-arm machine confirms that the fracture reduction is insufficient, the reduction is performed after using an auxiliary incision. We examined the protrusion and non-protrusion of the PFNA-II proximal nail from the tip of the greater trochanter. The 86 selected patients were divided into a herniated group (Group A) and a non-herniated group (Group B). The AO/OTA classification, blade position, Dorr type, reduction quality, etc. were analyzed based on X-ray films. According to the central position of the femoral neck on the postoperative anteroposterior radiograph of both hips, the position of the helical blade is divided into three types: upper, middle, and lower (Figure 1). In the protrusion group, the degree of protrusion of the PFNA-II nail on the lateral aspect of the greater trochanter was evaluated in the PACS system (Figure 2).
Result
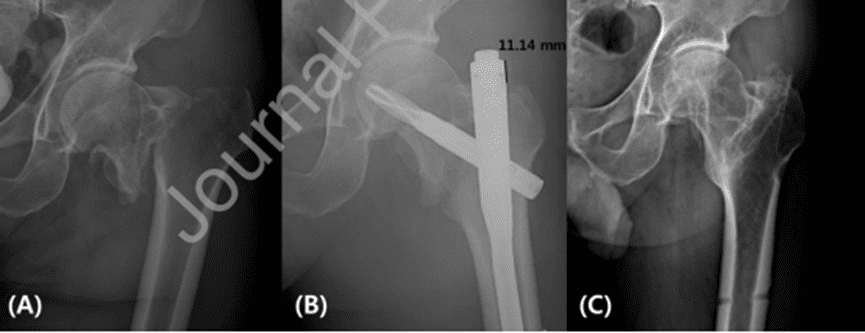
No differences were found in the demographic characteristics of the two groups. The average protrusion length of group A was 9.01mm, and that of group B was not protrusion. There was no statistically significant difference in the length and diameter of the main nail between the two groups. According to the postoperative anteroposterior radiograph of both hips, helical blades were implanted in 24 cases (80.0%) in the middle and 6 cases (20.0%) in the lower side of Group A, and in Group B, 31 cases (55.4%) were implanted in the middle and 25 cases (44.6%) on the lower side. In the analysis of the relationship between blade position and protrusion degree, the difference was statistically significant (P<0.037). The results showed that in group A, the spiral blade was implanted in the middle part of the femoral neck in 24 cases (80.0%) and in the lower part in 6 cases (20.0%); in group B, the helical blade was implanted in the middle part of the femoral neck in 31 cases (55.4%) and in the lower part in 25 cases. (44.6%), the difference was statistically significant (P<0.05). The average protrusion height when the blade was inserted into the center of the femoral neck was 9.03 mm, and when placed on the lower side of the femoral neck, the average protrusion height was 8.96 mm. There was no statistically significant difference between the two groups (see Table 2). Eleven of 30 cases (36.7%) in group A had significantly greater trochanter pain, and 6 of 56 cases (10.7%) in group B had significantly greater trochanter pain. The difference between the two groups was statistically significant (P <0.004). In group A, 2 of the 11 patients who complained of pain in the greater trochanter underwent internal fixation removal, and their symptoms disappeared after the operation (Figure 3). Based on this result, we speculated that the protrusion of the proximal PFNA caused postoperative pain to a certain extent.

Compared with Americans and Europeans, Asians have relatively short femurs and an excessively large anterior arch. In Asian patients, the procedure may be more challenging due to the potential risk of mismatch between PFNA design and proximal femoral anatomy. Typically, the surgeon determines the ideal nail length based on the patient’s femur size and fracture location. Although the length of the main staples is different, the design of the proximal portion inserted with a spiral blade is the same. Therefore, even if the main nail is inserted accurately after selecting a precise device, the proximal portion of the main nail may protrude in Asian patients with relatively small bony structures.
Conclusion
After surgical treatment of intertrochanteric fractures with PFNA-II, protrusion of the primary nail in the greater trochanteric region is common. The incidence of pain increases when the intramedullary nail extends beyond the greater trochanter. Therefore, we suggest that the PFNA be modified to further shorten the proximal segment suitable for Asian patients to achieve better clinical outcomes when treating intertrochanteric fractures.