 Skip to content
Skip to content
Introduction
Pilon fracture is a comminuted fracture of the distal tibia, accounting for approximately 1% to 10% of tibial fractures. Pilon fractures are caused by longitudinal axial loads that cause the talus to impact the articular surface of the distal tibia. The cortical bone fragments, metaphyseal cartilage and soft tissue fragments are compressed together by the impact force. Traumatic arthritis is a common sequelae due to severe fractures and destruction of joint surfaces.
Pilon is a French word that refers to a grinding rod or battering ram, a tool used for pounding or mashing. Étienne Destot introduced this term into orthopedic writings in 1911. Pilon fractures involve the articular surface of the distal tibia and the adjacent metaphysis, with or without involvement of the fibula. Management of this type of fracture can be challenging, especially when there is significant soft tissue damage. Although a variety of treatments are available for this type of fracture, timely and accurate surgery is important given the soft tissue condition.
The treatment of Pilon fractures has changed a lot in the past few decades. When internal fixation matured, surgery became mainstream and high-energy injuries and severe soft tissue injuries led to conservative treatment and external fixation as well as limited internal fixation. Return again.
As the importance of soft tissue and high versus low energy injuries become better understood, the outcome of treatment depends on the reconstruction of the joint and the condition of the soft tissue. Actual treatment concepts have also changed with the development of more advanced implants and surgical techniques.
Pathophysiology
Depends on the type of injury. Low-energy injuries result in minimal soft tissue damage. The fractures are minor, mostly spiral fractures with small displacement. High-energy injuries, such as falls from heights and high-speed car accidents. It can cause significant displacement and large comminuted fractures accompanied by severe soft tissue contusion, and can also cause open and contaminated wounds. It can also cause fractures of the fibula. Damage also occurs to the articular cartilage of the tibia and talus. The cartilage develops wear, bruising, or tears at the weight-bearing center of the tibia. Fragments from cartilage tears can become embedded in the metaphysis.
Treatment after admission
Don’t waste time in the emergency room; keep wounds covered with sterile dressings; get imaging done quickly. If possible, obtain the patient’s medical history and injury history (e.g., diabetes). Watch out for peripheral vascular disease and neuropathy.
The clinical manifestations of closed fractures vary depending on the severity of the injury and the time since the injury occurred. The soft tissue swells rapidly and the tension of the tissue increases, causing blisters. Multiple fracture fragments are severely displaced, thereby affecting the viability of the surrounding soft tissue sleeve. Crush injuries, skin degloving injuries, bruising, and hematomas can further damage soft tissue.
Keep the blisters caused by the fracture intact. Once it ruptures, it is likely to be infected by skin or hospital bacteria. Cephalosporins can be used for prophylactic anti-infective treatment. For highly contaminated wounds, aminoglycosides can be added.
In open fractures, photographs can be taken in a sterile room for documentation. Soft tissue injuries can be graded according to the Oestern/Tscherne or Gustilo scoring system.
Imaging manifestations
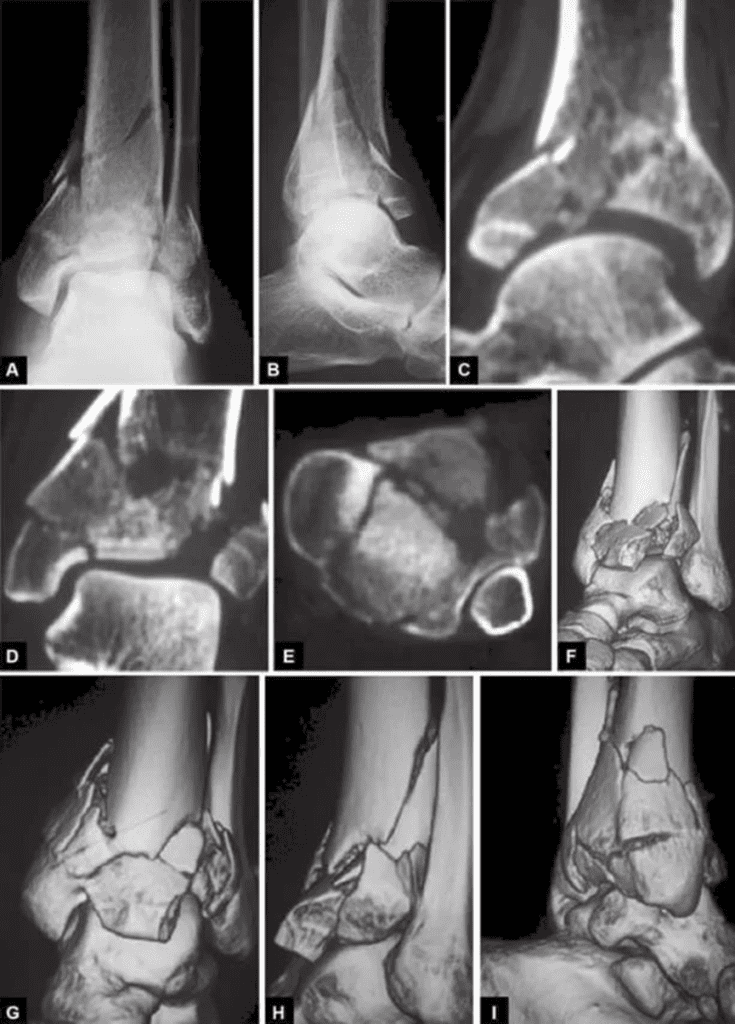
Plain X-rays, including anteroposterior, Mortise, and lateral views, provide comprehensive imaging of the ankle joint. CT scans and three-dimensional reconstructions of the distal tibia and ankle joint are almost mandatory to produce a more intuitive fracture model and better understand fracture fragment comminution, displacement, and embedding of joint fragments (Figure 1)
Types
The classification of AO/OTA is as follows (Figure 2 A~C)
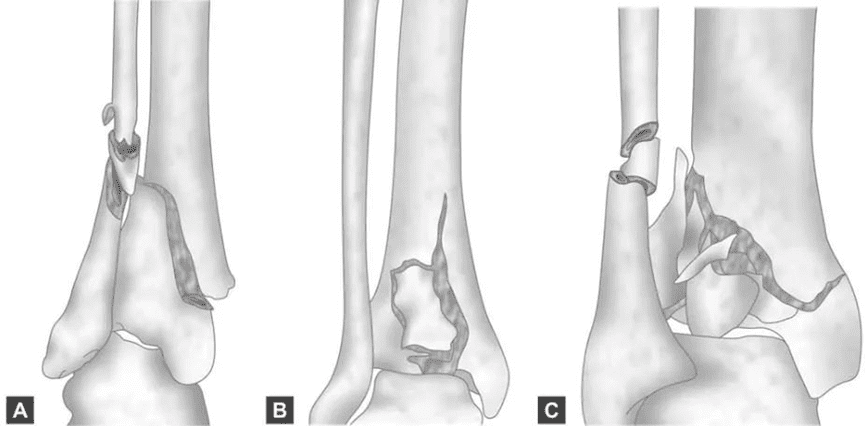
A~C AO/ATO classification Type A: Extra-articular fractures are divided into three subtypes: simple (A1), comminuted (A2), severely comminuted (A3); Type B: only involves part of the articular surface and one column, divided into three subtypes: simple split fracture (B1), split with collapse (B2), collapse and multiple fracture fragments (B3); Type C: involves the entire bone articular surface, divided into There are three subtypes: articular surface and metaphyseal fissure (C1), simple articular fissure with comminuted metaphyseal fracture (C2), and comminuted fracture of the articular surface and metaphysis (C3).
Type A: extra-articular fracture, divided into three subtypes: simple (A1), comminuted (A2), severely comminuted (A3)
Type B: only involves part of the joint surface and one column, and is divided into three subtypes: simple fissure (B1), fissure with collapse (B2), collapse and multiple fracture fragments (B3)
Type C: involves the entire bone articular surface and is divided into three subtypes: articular surface and metaphyseal clefts (C1), simple joint clefts with multiple bone fragments in the metaphysis (C2), and fractures with articular surface and metaphyseal fractures Multiple fracture fragments (C3)
Basic surgical instruments:
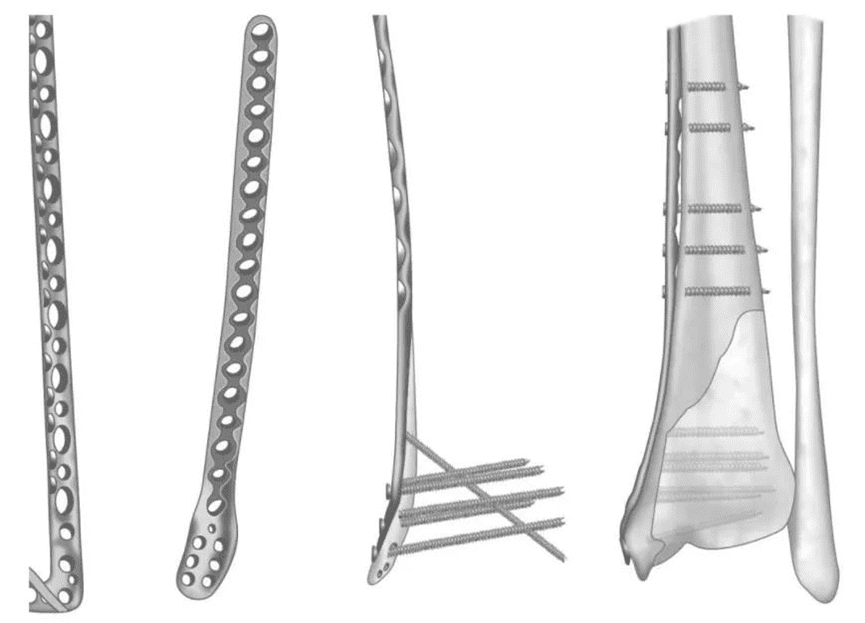
Reduction forceps; 1.8mm K-wires; 3.5mm screws (standard cortical and cancellous or self-tapping and tapping); 1/3 tubular plate for fibula; 3.5mm reconstruction plate (if Pilon requires support from both sides); 3.5mm dynamic compression plate (3.5DCP) on the medial aspect of the distal tibia can be used in place of the reconstruction plate; specially anatomically shaped distal tibial locking plates and screws (optional)
Surgical methods
1. Percutaneous or minimally invasive internal fixation
This technique can be applied to fractures with less displacement. Through closed needles or small incision exposure, K-wires are used as “push bolts” to reset the joint fragments. As soon as the fragment is reduced, cannulated screws can be inserted using fluoroscopic guidance.
External fixation aids can protect Pilon fractures after reduction. Arthroscopy can be used, but it is difficult because of narrow joint space and hematoma. External fixation can improve the alignment of fracture reduction, arthroscopy can help restore the articular surface, and minimally invasive screws can help stabilize the joint and protect soft tissue.
This method is not suitable for severely comminuted fractures and embedded fractures of joints.
2. External fixation
The immobilizer can span the ankle joint and work with the foot to provide stability to the reconstruction.
Two bone screws are placed at the upper end of the fractured tibia. The other is connected to the calcaneus through the calcaneus just below the tip of the lateral malleolus. The construct should be aligned with the central axis of the tibia to avoid subluxation of the joint.
Two 5mm bone screws are inserted into the proximal end of the tibial fracture from the sagittal plane, and the steel wire is placed 10 to 15mm above the joint bone, parallel to the joint. The direction of the wire is from posterolateral to anteromedial, and the strap can exert some pressure on the fracture. The bone screws and wires are connected by carbon fiber rods and rings. Take care to protect the peroneal tendon and sural nerve.
As a final treatment, this technique is only suitable for simple, indirect anatomically reduced intra-articular fracture types.
3. Open reduction and internal fixation
The fibula is first reduced and fixed, and a straight incision is made on the posterior edge of the fibula to avoid damage to the superficial peroneal nerve. Direct reduction of the fibula using sharp needle-nose forceps is generally not difficult. It is sufficient to use a 1/3 tubular plate with 5 or 6 holes for fixation. The plate is in a lateral or dorsolateral position. Complex fibula fractures are reduced by traction or indirectly with a small retractor (tension retractor). The steel plate used should be long enough for bridging and fixation.
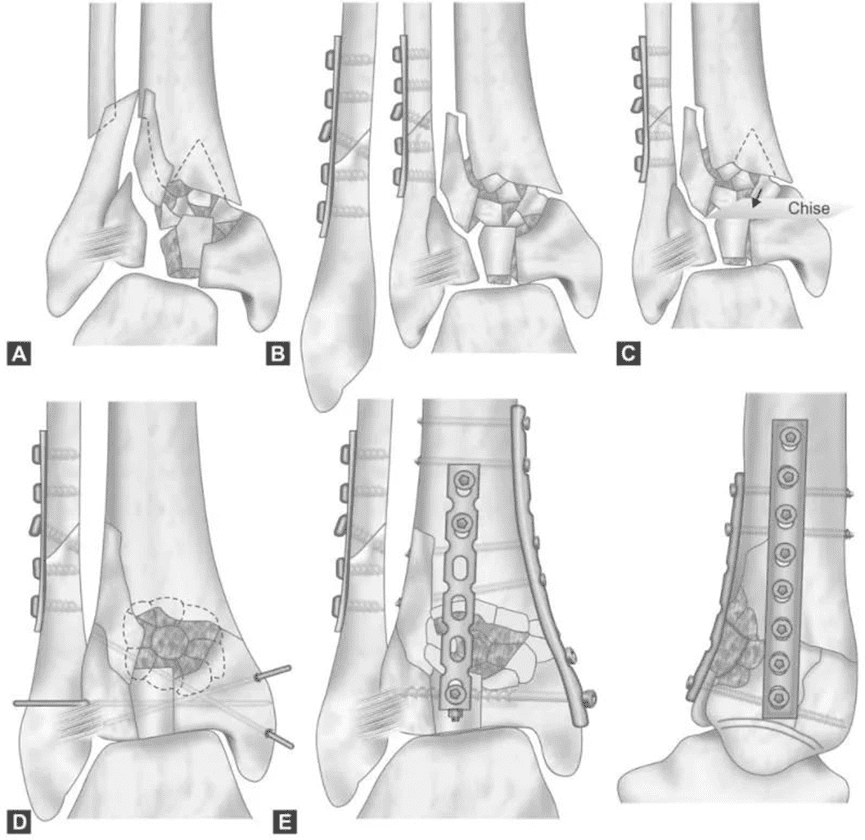
Reconstruction of the fibula facilitates the reduction of key lateral fragments of the tibia.
The distal tibia is exposed through an anteromedial incision overlying the distal tibia and slightly lateral to the anterior edge of the tibia along the tibialis anterior tendon. In patients with posteriorly displaced fractures, the posterolateral approach may also be used. In these cases, the fibula was repaired through the same approach.
The incision ends just below the medial malleolus. Pay attention to protect the superficial peroneal and saphenous nerves. Expose the fracture with minimal tissue dissection to avoid ischemia.
The joint must be opened from the front, paying attention to any damage to the cartilage. Gently lift the front piece and flip it aside. The centrally embedded metaphyseal fragment should be carefully and gently moved. The cartilage fragments are always extruded with the accompanying cancellous bone, and once the fragments are aligned, they are repaired with Kirschner wires. Sometimes point-type reduction clamps can achieve a good reduction effect.
Typically, a critical segment is the anterolateral syndesmotic segment, which must be well reduced and initially stabilized with 1 to 2 percutaneous K-wires. Fracture incisions should not damage the deep tibialis anterior artery.
After the joint is reduced, the cartilage fragments are also reduced and temporarily fixed with Kirschner wires and/or point reduction forceps. Results must be checked by fluoroscopy or X-ray
If the medial plate is insufficient to stabilize the fracture, two supports, one medial and one lateral, should be used.
Two reconstruction plates provide more stability compared to various designs of distal tibial plates, whether locking or nonlocking.
The tourniquet should be released before wound closure, leaving the fascia open. Place one or two drainage tubes. The skin is sutured tension-free using non-invasive techniques. If the fibula is repaired at the same time, the fibula wound can be left open due to tension issues and covered with a sterile dressing (such as polyurethane foam). After a few days, the wound is sutured a second time if possible.
While the patient is under anesthesia, a posterior below-knee splint is placed to maintain a neutral ankle position (90°). This prevents clubfoot from occurring.
Conclusion
Low-energy Pilon fractures have a good prognosis as long as the coordination of the joints is restored. In high-energy injuries and injuries caused by compression, early reconstruction and internal fixation are hindered due to damage to the soft tissue envelope. It is difficult to achieve good bony alignment with external fixation in these injuries. Therefore, post-traumatic arthritis is more likely to occur, and functional damage is more obvious. Post-traumatic ankle arthritis is more difficult to live with than other weight-bearing joints. This makes the less frequently performed ankle fusion a necessary solution. Comparison of results is difficult because of the variety of fracture patterns. There is a strong causal relationship between anatomical reduction and outcome, and the meticulousness of the surgery should be the biggest influencing factor on the outcome.