 Skip to content
Skip to content
Intramedullary nailing is widely used in trauma. If the intramedullary nail remains in the body and causes complications, surgical removal is usually required. However, the need for removal of asymptomatic or uncomplicated intramedullary nails remains controversial. This article will briefly describe the indications, methods and related complications of intramedullary nail removal.
Indications for intramedullary nail removal
Usually, the nail may need to be removed before the nonunion requires revision surgery. However, once the fracture has healed, removal of the nail becomes controversial. If persistent or progressive pain persists after the fracture has healed, nail removal may be indicated. Of course, before the etiology of the pain is clarified, removing the internal fixation blindly may not solve the problem, or even aggravate the problem. When deciding whether to remove the intramedullary nail, the surgeon should carefully consider whether the following indications exist.
1. Implant-related pain
Chronic pain after intramedullary nailing is common in the lower limb. For example, soft tissue irritation and impingement caused by protruding nail tails and protruding locking nail heads are definite sources of pain.
Pain at the greater trochanter after femoral antegrade intramedullary nailing is relatively common, but its exact incidence is still not counted, and this pain is often not caused by the protrusion of the nail tail. Pain in the front of the thigh may be caused by the tip of the intramedullary nail abutting the anterior cortex of the femur.
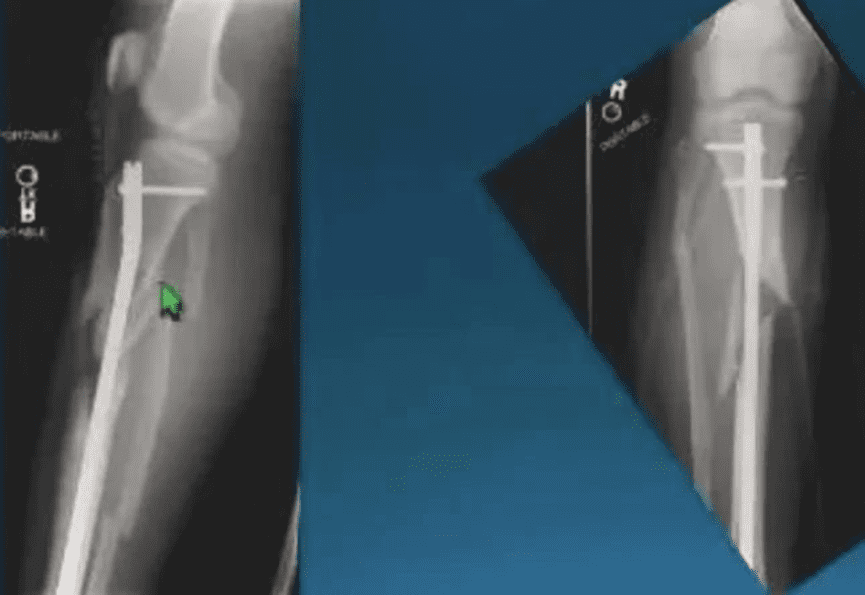
Anterior knee pain is also common after tibial intramedullary nailing. Pain occurs for many reasons, including disruption of normal anatomy during screw insertion (inferior patellar branch of saphenous nerve, patellar tendon, infrapatellar fat pad, medial meniscus, and tibial plateau or patellar cartilage).Anterior knee pain may also be caused by protruding nail tails at the entry point. Arthroscopy confirmed cartilage lesions caused by impingement of the protruding nail tail on the articular surface of the femur. At the same time, the protrusion of the nail tail can also cause damage to the patellar tendon. Indications for nail removal exist if protruding nail tails prove to be causing symptoms or complications.
2. The built-in is broken
Removing a broken intramedullary nail can be very challenging. Fixation failure is usually due to fatigue failure due to repeated threshold loading. During the secondary healing process of callus formation, the intramedullary nail is subjected to repeated deformation force stimulation. Compared with the early intramedullary nails with slots, the new closed-section intramedullary nails are more resistant to such deformation forces. Likewise, an increase in diameter can also improve the fatigue properties of the nail. Once the intramedullary nail is broken, it indicates that the fracture fragment is still mobile, so the broken intramedullary nail can be regarded as one of the signs of fracture nonunion; in this case, it is necessary to remove the intramedullary nail for further treatment.
Some physicians believe that the fracture of the interlocking screw is a manifestation of “automatic dynamics”, which is conducive to fracture healing. However, it should be clear that dynamization is only effective in order to increase the axial compression of the fracture site during the early healing process of simple fractures. In other cases, fracture of interlocking screws remains an indication for revision surgery.
3. Infection
The incidence of deep infection after intramedullary nailing for closed fractures is very low, about 1%. The infection rate after an open fracture can be as high as 17%. Deep infections often require removal of the intramedullary nail. It is beneficial to delay the removal of the nail and wait for the fracture to heal. However, infection after intramedullary nailing can significantly prolong the time to fracture healing, sometimes requiring debridement and revision before fracture healing occurs. The final thorough debridement should be performed after the intramedullary nail is removed, and the reaming operation can help remove the infected tissue.
4. Fracture nonunion
Once the diagnosis of nonunion is established, removal of the intramedullary nail should be considered before it breaks. Determining when the nail breaks is often difficult, so when to remove the nail is also controversial. However, it is much easier to remove a complete nail than a broken nail, so the surgeon must take this factor into consideration in subsequent treatment plans.

5. Subsequent joint replacement
Removing the nail many years after surgery can be difficult. The additional manipulation around the joint during joint replacement increases the risk of postoperative infection, and the complications of intramedullary nail removal complicate joint replacement surgery.
Neither shaft fracture nor intramedullary nailing was a risk factor for subsequent arthroplasty, whereas intra-articular trauma was a risk factor for arthroplasty. Patients with inflammatory joint disease may also subsequently require joint replacement therapy.
Complications of intramedullary nail removal
The complications of intramedullary nail removal include delayed wound healing, infection, subsequent soft tissue injury, refracture, new pain symptoms, inability to relieve existing pain, and failure to remove the internal fixation. The incidence of complications varies according to the anatomical site.
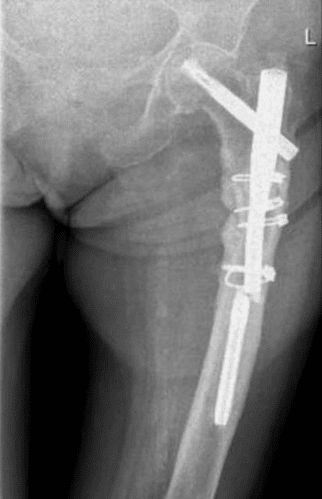
1. Femur
There are a few complications in the removal of the femur. Such as Hematoma formation after internal fixation removal and intramedullary nail breakage is difficult to remove.
2. Tibia
The complication rate after tibia intramedullary nail removal is about 10%. Complications include failure to remove, intraoperative fractures, and incision infection. About half of the patients were required to bear weight with the help of crutches after removing the intramedullary nail, and these patients could fully bear weight before the operation. In about 25% of patients, the pain was not relieved or even aggravated after the intramedullary nail was removed.
3. Children
As a special group in intramedullary nail surgery, children use different intramedullary nails from adults. The removal of the elastic intramedullary nail is relatively safe and has fewer complications, about 7%. If removing the forearm intramedullary nail prematurely, the probability of recurrent fracture is higher.
Surgical technique
Removal of the intramedullary nail is a routine operation, manufacturers will provide corresponding instruments. Once the intramedullary nail breaks, the situation becomes particularly difficult. At this time, special instruments and skills are required to remove the intramedullary nail.
The order in which the nails are removed is critical. Before removing the internal fixation, the nail tail must first be found and grasped. End caps are sometimes difficult to see on radiographs, and for this reason, some physicians do not recommend the use of end caps unless they increase the working length of the nail.
After taking out the tail cap, use the guide arm to grasp the intramedullary nail, and then perform the locking nail removal operation. It must be borne in mind that all locking screws must be removed before attempting to remove the main nail. If an exact fit is not possible, the option to use a tapered extraction tool may aid in grasping the caudal end of the nail. If bone in growth in the nail hole or on the surface of the nail is suspected, the nail can be driven a few millimeters inward with a slide hammer before removal.
If it is necessary to open the broken end of the fracture for cleaning and reduction, the intramedullary nail can be removed through the broken end. Below, we will briefly introduce some extraction methods that do not require exposing the fracture ends.
1. Remove the broken cannulated intramedullary nail
Usually, it is not very difficult to remove the proximal portion of a broken intramedullary nail. Once the proximal part is removed, it becomes a challenge to remove the distal part without opening the fracture. Reaming to enlarge the proximal medullary canal by a few millimeters may facilitate distal screw removal.
The distal portion can sometimes be grasped and successfully removed using long forceps. However, the long forceps cannot provide a strong grip, and the successful removal depends on whether the distal part is loose.
Driving a thinner intramedullary nail or a manual awl drill into the distal broken nail also sometimes facilitates its removal. During the driving process, the distal locking nail should be retained to avoid further displacement of the distal part during driving. Once is securely bonded to the distal portion, remove the distal locking nail, and the distal portion is then knocked back to remove the broken nail.
Finally, if all of the above techniques for proximal removal have been unsuccessful, distal removal of the nail can be attempted.
For example, through the knee joint, through the opening of the distal femur, remove the distal part of the broken intramedullary femoral nail. The drill hole is directed toward the distal end of the nail, and the opening is large enough to accommodate an olive-tipped guide wire with a washer. Pass the guide wire retrogradely through the cannulated of the intramedullary nail and protrude from the opening of the proximal femur, and the olive head with spacer can bring the broken distal nail out of the proximal femur.
A similar technique can be used for the tibia, where the distal opening of the guide wire is placed retrogradely at the medial malleolus. Sometimes, inserting a guide wire through the opening and knocking against the distal broken nail can move the broken nail a little proximally, which is helpful for retrograde insertion of the guide wire and removal of the broken nail.
2. Remove the broken solid intramedullary nail
Solid intramedullary nails are generally more difficult to remove than cannulated intramedullary nails. The extraction technique includes reaming of the proximal medullary canal and effective grasping of the distal broken nail. Laparoscopic claws can be used for grasping distal broken nails. However, using various tools may not be able to effectively grasp the distal broken nail. At this time, the broken nail has to be knocked out from the other end of the bone. The technical principle is similar to that of the cannulated intramedullary nail. Use tools such as soft drills and hard guide wires to knock out the broken nails from the distal end directly to the proximal end.
3. Remove the broken interlocking screw
The head or proximal portion of an interlocking screw can usually be removed with the supplied screwdriver. Sometimes the threads of an interlocking screw slip in the bone, requiring traction with pliers around the screw head while a screwdriver is used to unscrew it. Damaged screw heads may require special tools for removal, such as internal fixation removal kits such as counter-thread drills. The distal part of the broken screw is sometimes completely loosened, which does not affect the removal of the main nail, and can be left in the body if it does not affect subsequent treatment operations. However, sometimes a broken distal nail will cause an iatrogenic fracture during removal of the main nail, at which point it will be necessary to remove it.
The most commonly used method is the push-out technique of the screw, that is, the main nail is retracted to its original position, so that the nail hole on the bone surface is in the same line as the locking hole of the intramedullary nail, and the broken bone is screwed out. Use a guide wire, a small hammer rod, or a screwdriver. The staples are pushed out through the staple holes in the contralateral cortex and removed through a separate incision.
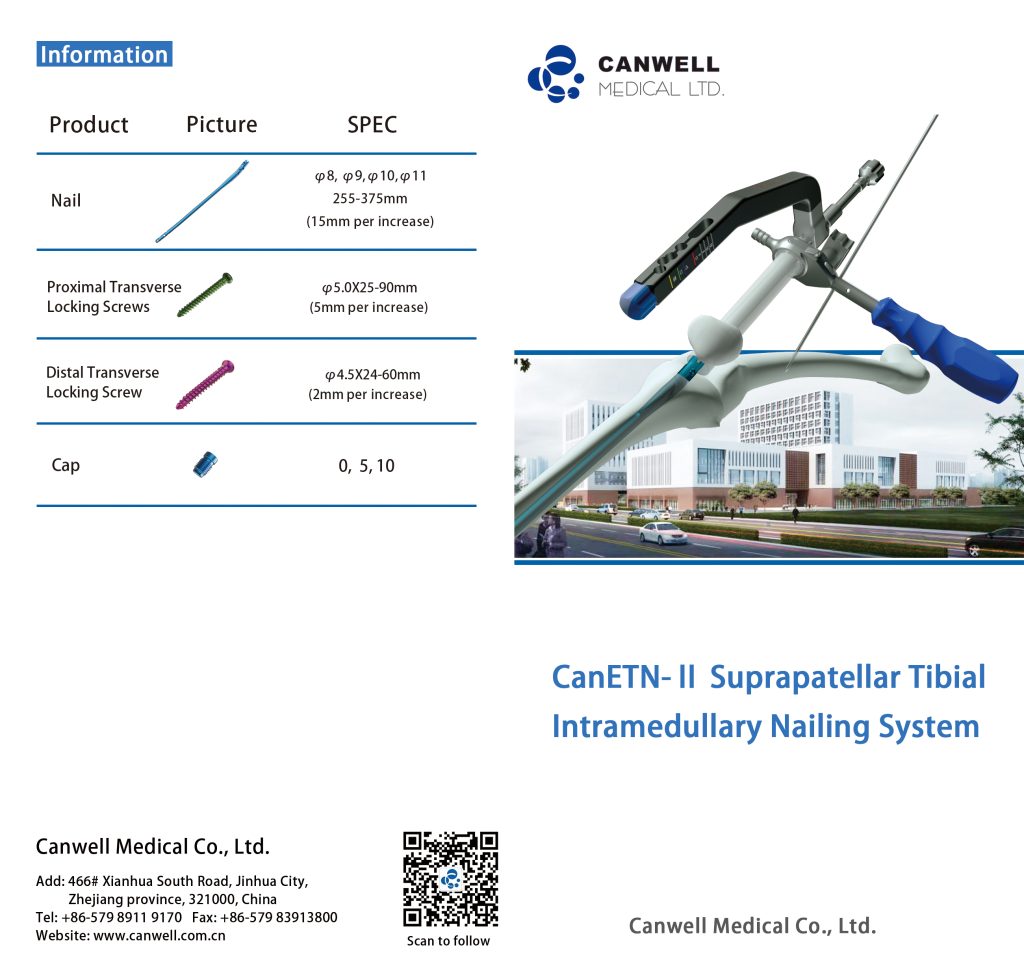
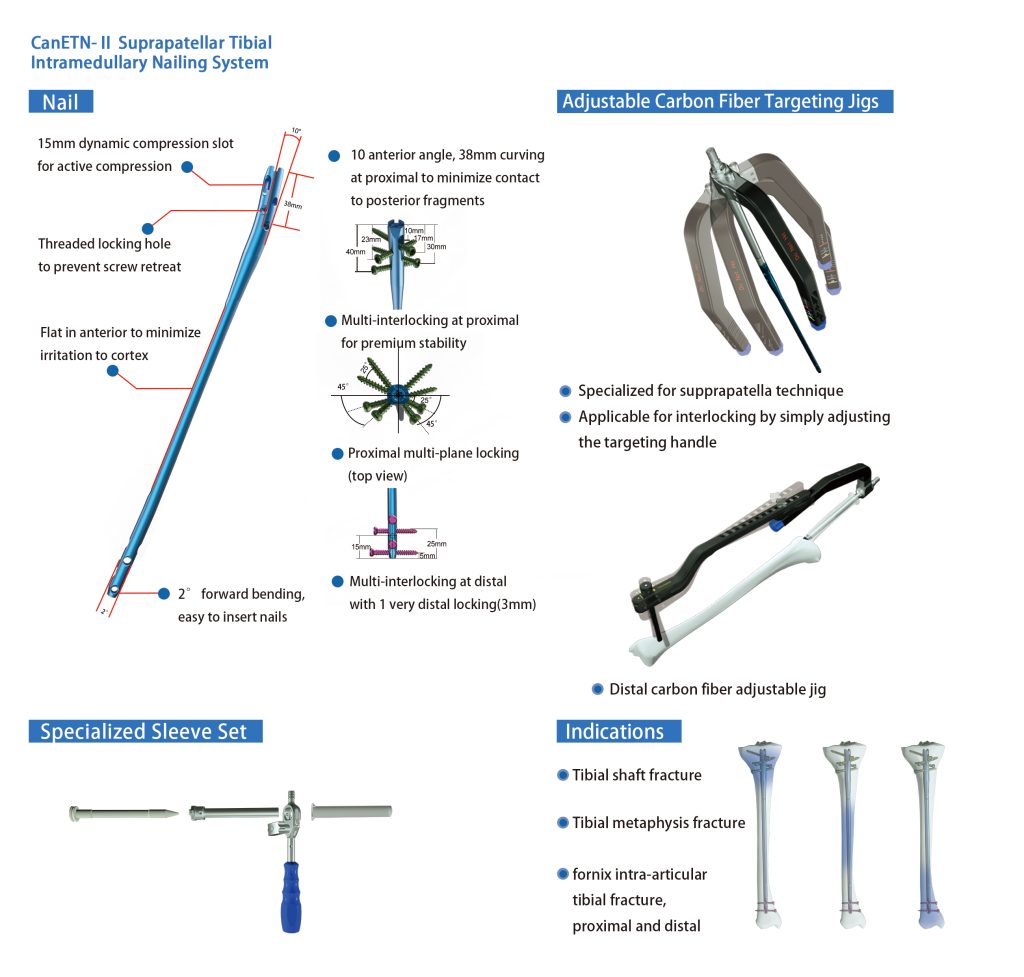
Canwell Tibia Intramedullary Nail– CanETN-II
The CanETN- II, the pinnacle of orthopedic innovation for tibia fracture management. With a 15mm dynamic compression slot for active compression, a threaded locking hole to prevent screw retreat, and a flat anterior surface to minimize irritation, it offers unprecedented surgical precision. Its 10° anterior angle and 38mm proximal curve minimize contact with posterior fragments, while multi-interlocking systems at both proximal and distal ends ensure premium stability. The CanETN- II is specialized for suprapatellar techniques and can adapt easily with its adjustable targeting handle. Indicated for tibia shaft fractures, tibia metaphysis fractures, and fornix intra-articular tibia fractures, this revolutionary solution provides the ultimate support for orthopedic surgeons seeking optimal outcomes in tibia fracture care. Elevate your practice with CanETN- II, where precision meets stability for superior patient results.
Summary
Persistent pain after fracture healing is often one of the indications for intramedullary nail removal. The removal of the intramedullary nail, whether it is a complete intramedullary nail or a broken intramedullary nail, has corresponding risks and difficulties, and the removal operation is often more invasive and complicated than the intramedullary nail insertion. Surgeons and patients must carefully evaluate and discuss whether this procedure can actually solve the problem.