 Skip to content
Skip to content
When winter comes, many people will choose various snow activities such as skiing. At the same time, various injuries caused by skiing appear. Relevant data shows that about 100,000 people are injured every year due to skiing. This article combines multiple documents and relevant statistics to summarize and organize the conventional treatment methods for three types of ski injuries.
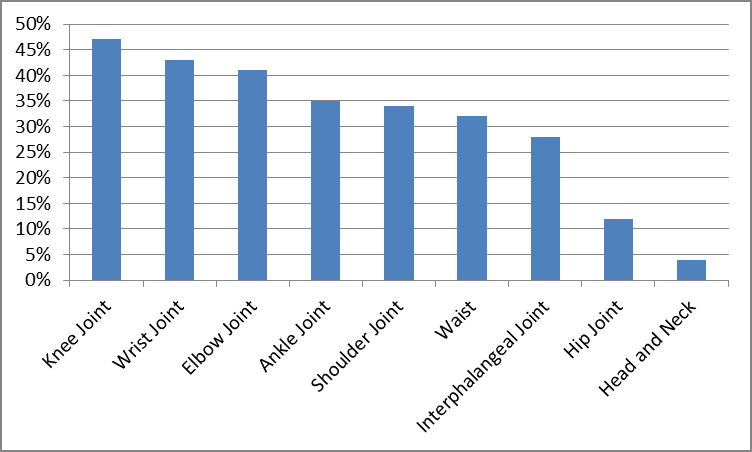
Percentage of various sports injuries
Common sports injury locations in snow sports are knee joint (47%), wrist joint (43%), elbow joint (41%), ankle joint (35%), shoulder joint (34%), waist (32%), interphalangeal joints (28%), hip joints (12%), and head and neck (4%) (see Figure 1). Skiers’ sports injuries are mainly distributed in the limbs, among which knee joint injuries are the most common. The main reason is related to skiing. The movement requirements are related to the joint angles of the participants, as well as the body posture and force generation method during skiing.
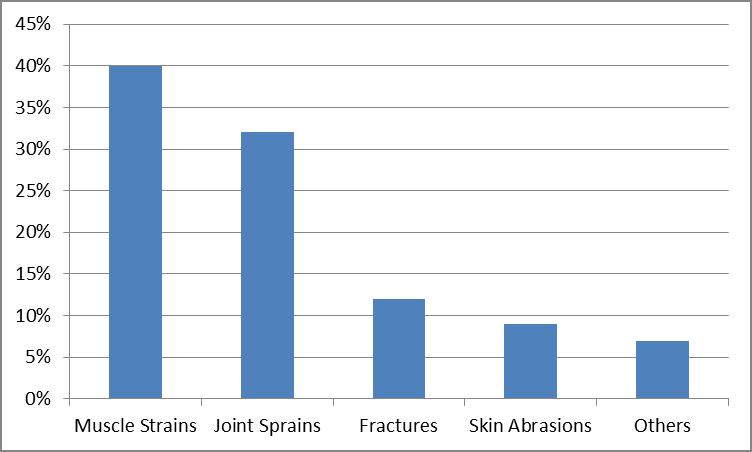
Common types of sports injuries in snow sports are muscle strains (40%), joint sprains (32%), fractures (12%), skin abrasions (9), and others (7%) (see Figure 2). Most snow sports injuries are compound injuries, containing two to three types of injuries at the same time, which require higher requirements for subsequent treatment and rehabilitation. The main reason for the injury is that the skier is unable to complete body control and balance during exercise, and eventually falls due to the shift of the center of gravity to an angle that cannot be adjusted.
Inadequate body control occurs due to the following conditions:
(1) Sufficient preparatory activities are not carried out before exercise, the muscles are not yet in an excited state, and the muscle contraction force is insufficient or decreased, which triggers a series of reactions, thereby increasing the chance of injury during exercise.
(2) The intensity during exercise is too high, and the body function is limited and unable to meet the intensity requirements of the exercise, resulting in insufficient body control during exercise and sports injuries.
(3) There is no relaxation activity after exercise. Relaxation training, as an indispensable part of the exercise process, is often ignored by people, causing people to return directly from the state of strenuous exercise to a calm state, which not only increases the cardiovascular burden, but also causes Lactic acid accumulates in the muscles, causing muscle fatigue and, in severe cases, muscle damage.
Common damage treatment methods
1. Ligament injury
Due to deceleration and steering movements during snow sports, the knee joint twists, and shear stress occurs throughout the process, leading to anterior cruciate ligament injury, medial collateral ligament injury, etc.
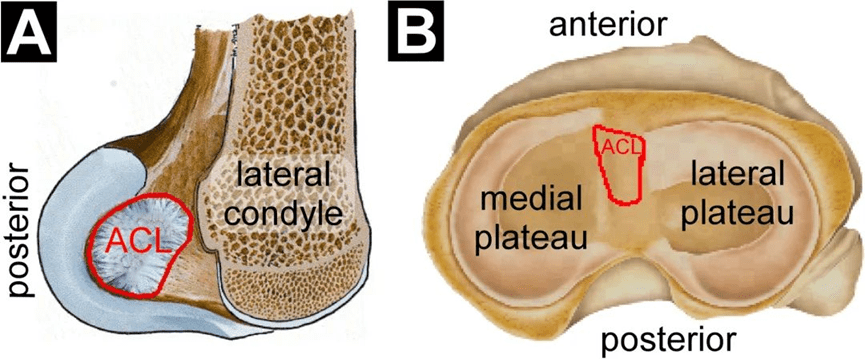
1.1 Anterior Cruciate Ligament Injury
The anterior cruciate ligament originates from the anterior depression of the medial intercondylar ridge of the tibial plateau and is connected to the anterior horn of the lateral meniscus. It runs upward, posteriorly and laterally in a fan-shaped manner, and ends at the medial surface of the lateral femoral condyle (see Figure 3). Due to external force, violence and other factors, the continuity of the anterior cruciate ligament is destroyed, and tearing or even rupture occurs. The main symptoms of patients with acute injuries are tearing sounds, pain, swelling, and limited joint movement of the knee joint; those with chronic injuries the main symptoms of patients are joint instability and joint dislocation. Snow sports often cause acute anterior cruciate ligament injuries, which are non-contact injuries and require conservative or surgical treatment depending on the injury.
(1) Diagnostic examination:
Drawer test, Lachman test, lever test, joint X-ray examination, joint MRI, etc.
(2) Conservative treatment:
Wearing knee braces, using crutches, and performing rehabilitation exercises in daily life can help reduce pain and swelling, restore knee joint function, enhance muscle strength and joint stability, and prevent secondary injuries.
(3) Drug treatment:
Oral non-self-extracting anti-inflammatory drugs can help patients reduce pain and swelling and eliminate inflammation. Commonly used drugs include Celebrex, etoricoxib, etc. An appropriate amount of steroid drugs are injected into the joint cavity to relieve pain.
(4) Surgical treatment:
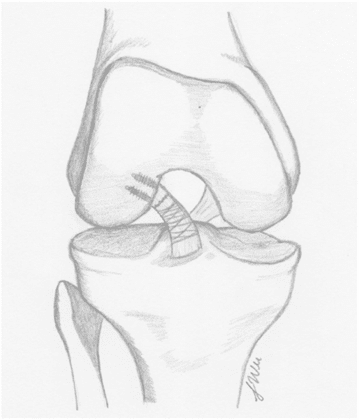
Suture anchor repair (SAR): Relying on the innate healing ability of the native ACL, the autogenous ACL is repaired and anchored in the femur without the need for additional structural reinforcement (see Figure 4). Suitable for Sherman type 1 proximal tears, other tissue quality is excellent.
Internal Bracing (IBLA): Utilizing innovative synthetic materials to provide additional strength to the healing tissue, new materials are used as an internal scaffold within the repaired ACL (see Figure 5). Indicated for primary repair of ruptured anterior cruciate ligament, type 1 proximal rupture with good tissue quality.
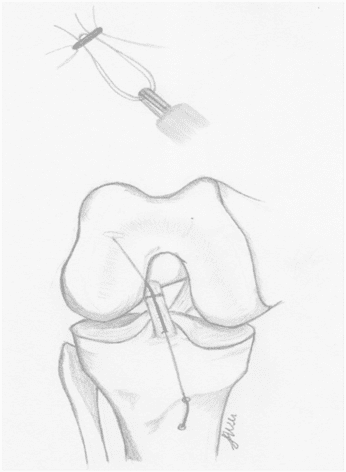
Dynamic intraligamentous stabilization (DIS): consists of a tibial preload spring that tightens the torn anterior cruciate ligament and narrows the bony suture line with the femoral footprint (see Figure 6). Applicable to any tear classification, including mid-layer material rupture, but occurs in 4-15% of patients.
Bridge-enhanced anterior cruciate ligament repair (BEAR): enhances the adverse healing response of the native ACL through a collagen bioscaffold, optimizes clot formation and cytokine release, and promotes ACL healing (see Figure 7)
2. Medial collateral ligament injury
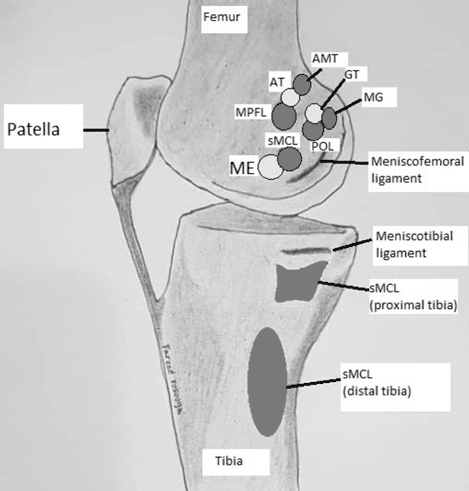
The medial collateral ligament originates from the medial condyle of the femur and ends at the tibial plateau. It stabilizes the medial side of the knee joint (see Figure 8). Under the action of valgus force, the medial ligament of the knee joint is damaged. Common symptoms include pain, swelling, and knee instability on the inside of the knee.
(1) Diagnostic examination:
Range of motion, swelling and tenderness examination, X-ray examination, MRI examination
(2) Conservative treatment:
Rest at home, apply ice to eliminate swelling and relieve pain, take anti-inflammatory drugs as recommended by your doctor, and use crutches and braces to ensure adequate protection of the knee joint. Combined with the actual situation, rehabilitation exercises are carried out according to the doctor’s recommendations and are suitable for patients with level 1 to 3 injuries.
(3) Surgical treatment:
Patients who meet the surgical indications undergo medial collateral ligament reconstruction surgery.
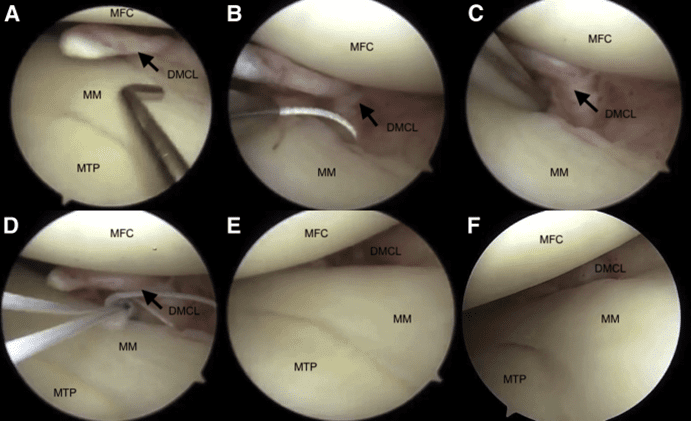
Femoral tear: pass through the meniscus above the meniscal capsule junction from the inside out, and suture repair according to the preoperative plan (see Figure 9).
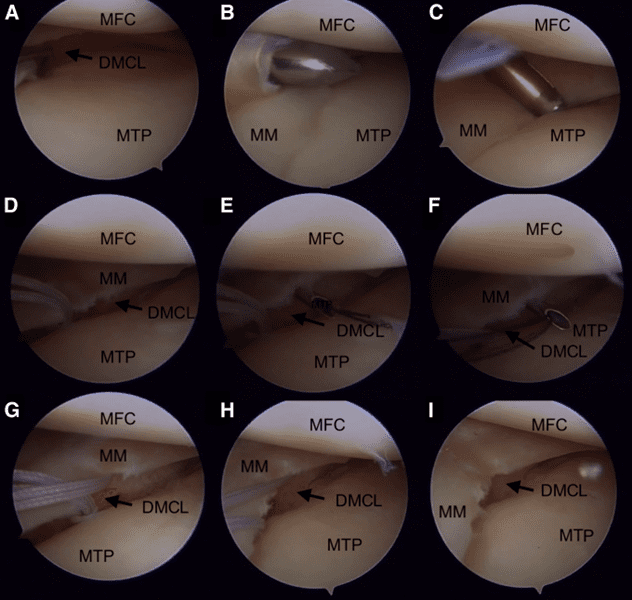
Tibial tear: Enter the tibial side close to the DMCL, and the suture thread passes through the torn medial tibial collateral ligament fibers, and is sutured and repaired according to the preoperative plan (see Figure 10).
3. Meniscus injury
The meniscus is located between the femur and tibia. It is a cushioning structure composed of elastic cartilage that can cushion the joint surface and prevent damage caused by impact. When performing snow sports, the knee joint is in a flexed position, accompanied by internal and external rotation of the knee joint. Because the movement exceeds the normal range of joint motion, a meniscus tear can occur. Common clinical symptoms are pain, swelling, snapping and interlocking of the knee joint.
(1) Diagnostic examination:
McMurray joint tenderness test, MRI examination, arthroscopy, MRA examination
(2) Conservative treatment:
Focusing on symptom management, analgesics, non-steroidal anti-inflammatory drugs and ice packs are used to reduce pain and swelling based on the patient’s own symptoms and the doctor’s judgment.
(3) Surgical treatment:
Microscopic meniscectomy: Use arthroscopy to remove all menisci. This option will increase the peak pressure of tibial-femoral contact, reduce the contact area, and will also cause the rapid progression of osteoarthritis. Indicated for patients with severe pain, locking and other mechanical changes, as well as patients with severe chondromalacia and arthritis.
Figure 13: A complex tear of the medial meniscus seen from an anterolateral view. b View of a complex tear after meniscectomy. c View from the anteromedial portal showing a split tear of the lateral meniscus. d View of the tear after meniscectomy.
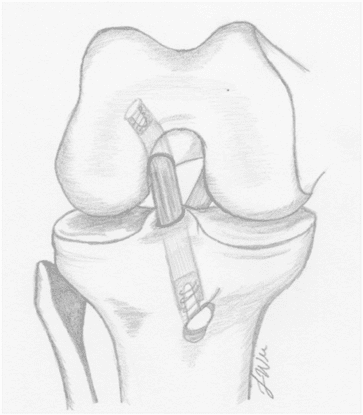
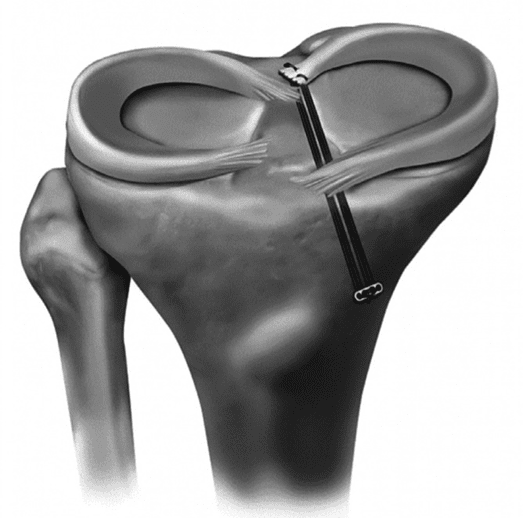
Meniscal repair: The most common technique is tibial pull-out repair, in which one or two tunnels are drilled from the anterior proximal aspect of the tibia through the anatomic attachment site of the torn meniscus, and the tear is then sutured through The tibial tunnel is removed, the sutures are tightened, and the meniscus is restored to its anatomical position. (See Figure 11).
4. Fracture
Tibial plateau fracture
The proximal end of the tibia has two condyles, with a smooth upper surface as the articular surface, and a tuberosity in front as the attachment point of the patellar ligament. Due to external impact, the joint is twisted beyond the range of motion, and sports on snow can easily cause tibial plateau fractures, most of which are oblique or spiral fractures. Common clinical manifestations include joint swelling and pain, mobility impairment, and intra-articular hemorrhage.
(1) Diagnostic examination
X-ray examination, CT examination, bone fricative examination, MRI examination.
(2) Conservative treatment:
It is suitable for fractures where the tibial edge fragment is not dislocated or has minor dislocation. Based on the examination results, it is judged whether the indications for conservative treatment are met, plaster immobilization, bone traction combined with drug treatment are adopted, and rehabilitation training is carried out according to the doctor’s requirements.
(3) Surgical treatment:
Arthroscopic reduction and internal fixation (ARIF): Repair and fixation of the intra-articular tibia through arthroscopically assisted surgery, suitable for non-dislocation or nearly dislocation split fractures, depression in the mid-joint or posterior joint area, and avulsion of the intercondylar eminence Fracture
Closed reduction and percutaneous fixation (CRIF): Percutaneous cannulated screw fixation is suitable for osteosynthesis of simple fractures without large bone defects. The latest balloon tibioplasty is a minimally invasive technique that is different from arthroscopy and is still in the experimental stage.
Open reduction and internal fixation (ORIF): suitable for complex fractures with multiple injuries.
tibial diaphysis fracture
During snow sports, due to external impacts, falls, collisions, etc., the tibial diaphysis is continuously broken. Common clinical symptoms are calf swelling and pain, accompanied by deformity and abnormal mobility.
(1) Diagnostic examination: same as tibial plateau fracture examination
(2) Conservative treatment:
Indicated for incomplete fractures, stress fractures, and undisplaced or lightly displaced fractures due to low-energy trauma. Use splint fixation, plaster fixation or other external fixation methods, as well as drug treatment and rehabilitation treatment.
(3) Surgical treatment:
Intramedullary nail fixation (IMN): Assess the width of the narrowest part of the tibial medullary canal, determine the entry point of the intramedullary nail, and use the patellar tendon or parapatellar tendon approach.
Plate osteosynthesis (MIPO): It is suitable for displaced and unstable fractures on the tibial side and the middle and lower 1/3 of the distal tibial shaft. It can be performed with or without involving the articular surface. The fracture site is reduced and fixed with a steel plate, making sure that the steel plate is covered by soft tissue during the operation.
External fixation: suitable for open fractures and soft tissue defects, acute shortening of limbs, and can also be used for later distraction osteogenesis.